What is thyroid cancer?
The high incidence and mortality rate of cancer in our lives make us fearful of "cancer", but thyroid cancer is called "lazy cancer" and "happy cancer". Famous Hong Kong movie star Liza Wang and badminton player Wang Nan both had thyroid cancer and recovered well after surgery.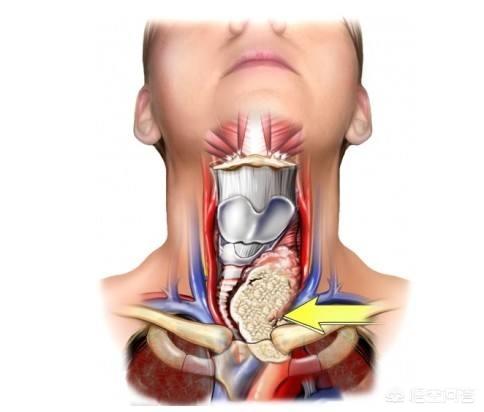
First of all, thyroid cancer is called "lazy cancer" because of its low degree of malignancy. Most of the patients go to the hospital for checkups after unintentionally discovering lumps in the front of the neck or enlarged lymph nodes in the neck, and usually the patients can survive with the tumor for several years without any symptoms.
Secondly, the imaging technology represented by ultrasound has greatly improved the detection rate of thyroid cancer. In recent years, with the increasing popularity of medical checkups and the wide use of thyroid ultrasound in medical checkups, the detection rate of thyroid cancer, especially the tiny thyroid cancer less than 1 centimeter, has become higher and higher. Patients with early stage of thyroid cancer, after timely treatment, can generally obtain more satisfactory treatment results and have better prognosis. Therefore, some people jokingly say that thyroid cancer is the happiest cancer, and if a person has to get one kind of cancer in his life, he would like it to be thyroid cancer.
About 90% of thyroid cancer can be treated by surgery, and patients with clean surgical resection do not need further chemotherapy and radiotherapy, but still need endocrine treatment. After standardized treatment, the 5-year survival rate of thyroid cancer patients is 88.5%, among which the 5-year survival rate of women is 92.8% and that of men is 75.4%. 20-year survival rate of non-advanced thyroid cancer patients under the age of 45 years can reach 85% to 90%. Since radiation or chemotherapy is not effective for most thyroid cancers, thyroid cancer is still mainly treated by surgery. Whether thyroid cancer recurs or metastasizes after surgery is obviously related to the scope of surgical resection. According to statistics, the recurrence rate after simple tumor resection is 40%-60%, the recurrence rate after resection of tumor and its affected thyroid lobe is 20%-30%, and the recurrence rate after combined radical neck surgery is 10%-20%. In addition, the degree of malignancy of thyroid cancer also determines the recurrence rate, that is to say, the higher the degree of malignancy, the higher the possibility of postoperative recurrence or distant metastasis. The recovery period from 0 to 3 years after treatment is the peak period of tumor recurrence and metastasis, and it is necessary to check on time during this period.
The current guidelines for the diagnosis and treatment of thyroid diseases in the U.S., Europe, Asia and other countries/regions are divided on the treatment strategy for papillary microcarcinoma of the thyroid, with the European guidelines advocating surgical resection, while the guidelines in the U.S. and Japan tend to favor active follow-up and surveillance of very low-risk papillary microcarcinoma rather than necessarily surgery. Therefore, there is no good method to determine whether a nodule is "very low risk", and this should be the focus of future research.
As a former thyroid surgeon, I'm happy to answer questions in my area of expertise.
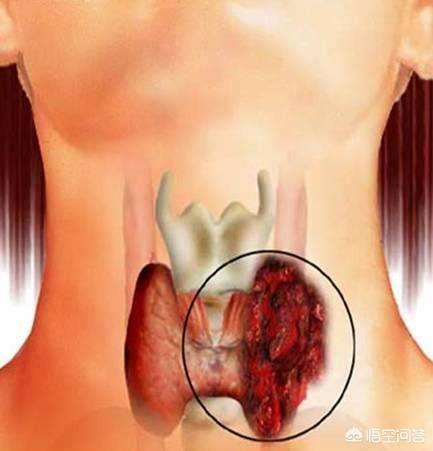
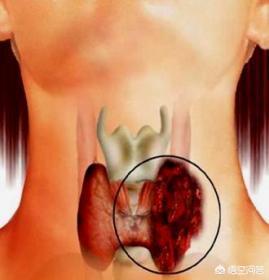
The thyroid gland is an organ of the body that grows in the neck position of the body. Thyroid cancer, as the name suggests, is cancer that grows on the thyroid gland.
Thyroid cancer can be divided into four types: papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC), medullary thyroid carcinoma (MTC), and undifferentiated thyroid carcinoma (ATC). Among them, PTC and FTC are relatively less malignant carcinomas with better prognosis, while MTC and ATC are relatively more malignant carcinomas with worse prognosis.
About 90% of all thyroid cancers are PTC, and PTC has almost certainly the best prognosis of all cancers. The vast majority of PTC (with lymph node metastasis confined to the neck) can be surgically resected completely, and supplemented by postoperative iodine 131 treatment, the probability of postoperative recurrence can be reduced to a very low level.
However, PTC should not be taken lightly because of this, and no matter how good the prognosis of papillary thyroid cancer is, it still carries the word "cancer", and recurrence and metastasis are the common features of all cancers, and PTC may also metastasize to important organs such as the liver, lungs, and bones. PTC may also metastasize to important organs such as liver, lungs, bones, etc. Patients who passed away due to PTC can be seen from time to time, and it is totally wrong for some public platforms to say that "papillary thyroid cancer is not considered as cancer".
① I am a former thyroid surgeon with a master's degree in clinical medicine, specializing in the diagnosis and treatment of thyroid diseases. If someone wants to consult the condition, you can communicate with me by private message, which will be more detailed and serious than the busy clinician's answer. ③ My public number (health knowledge workshop), published a variety of medical health knowledge (including: thyroid knowledge, all kinds of medical health knowledge, etc.), welcome to pay attention.
According to the latest national malignant tumor incidence and mortality data, among women, the incidence of major malignant tumors in the country's top ten, of which thyroid cancer is in the fourth place, in 2014, the incidence of thyroid cancer in women was 7.50%, and in 2015 it was 8.49%, which is evident that the incidence of thyroid cancer has increased. Some people think that thyroid cancer is relatively "kind" compared to other cancers, and many of them can be cured or do not affect life expectancy, but this is cancer after all, we can not generalize, and this is the overall data, so thyroid cancer patients still need to pay attention to.
What is thyroid cancer?
High risk groups for thyroid cancer:
For high-risk groups, it is more important to pay attention to the thyroid gland and be alert to thyroid cancer. The high-risk groups for thyroid cancer include the following: (1) people with a history of head and neck radiation exposure or radioactive dust exposure during childhood. (2) People with a history of systemic radiation therapy, (3) People with a past or family history of differentiated thyroid cancer, medullary thyroid carcinoma or multiple endocrine neoplasia type 2 (MEN2), familial polyposis, and certain thyroid cancer syndromes (e.g., multiple dysgraphism syndrome, Carney syndrome, Werner's syndrome, Gardner's syndrome).
Common symptoms of thyroid cancer:
Most patients with thyroid cancer do not have obvious symptoms, but usually find small lumps in the thyroid gland during palpation or ultrasound examination. If thyroid cancer is combined with thyroid function abnormality, it may show symptoms related to thyroid function abnormality, such as hyperthyroidism, hypothyroidism and so on. If thyroid cancer presses on organs and tissues such as esophagus and trachea, it can lead to adverse reactions such as difficulty in swallowing, hoarseness and difficulty in breathing. For medullary thyroid cancer, since the tumor itself can produce calcitonin and 5-hydroxytryptamine, it can cause patients to have diarrhea, palpitations as well as flushing and other symptoms. Therefore, if you have diarrhea for a long time and can't find the cause, you can go to check the thyroid gland to exclude the possibility of thyroid cancer.

Common treatments for thyroid cancer:
First of all, let me introduce you to what is the thyroid gland?The thyroid is one of the more important glands in vertebrates and it is an endocrine organ. The thyroid gland relies on the production of thyroxine to regulate the rate at which it is used to control energy, to make proteins, and to be sensitive to other hormones in the body. The average adult thyroid weighs 20 to 40 grams and is butterfly-shaped, resembling a shielded armor, hence its name.
Thyroid cancer is the most common malignant tumor of the endocrine system, with four times as many female patients as male patients. It is divided into four main categories:Papillary carcinoma, follicular carcinoma, undifferentiated carcinoma, medullary carcinomaNine of them are papillary carcinomas, which have a relatively good outcome after surgery. Ninety percent of these are papillary carcinomas, all of which have relatively good outcomes after surgery.
Symptoms in patients with thyroid cancerThyroid lumps that have been present for many years or that have rapidly increased in size over a short period of time; hoarseness, difficulty breathing and swallowing, and significant compression symptoms.
Common causes of morbidity:
1. Both iodine deficiency and high iodine diets may promote the incidence of thyroid cancer. However, opinions are not yet uniform.
2. Radiation can deform cell nuclei, cause problems with thyroxine secretion, and lead to cancer.
3, other thyroid diseases, such as thyroid hyperplasia, hyperthyroidism, nodular goiter and other patients, there are also chances of combining with thyroid cancer.
4、Family genetic factors, clinically, it can also be seen that more than two members of a family have papillary cancer.
The common treatment for thyroid adenocarcinoma is surgery to remove the affected area, up to total removal of the thyroid gland. Relatively low lethality and longer average survival time after surgical treatment.
I hope my answer is beneficial to my patients and I wish you good health.
focus"A Beautiful Pharmacist for Your Health, let the beautiful pharmacist accompany you on your journey to health.
Choose authoritative science, enjoy a healthy life, welcome to follow the MD team!
 thyroid cancerIt is the most common malignant tumor of the thyroid gland, accounting for about one-third of all malignant tumors in the body.1%. These include the following
thyroid cancerIt is the most common malignant tumor of the thyroid gland, accounting for about one-third of all malignant tumors in the body.1%. These include the following
- Papillary carcinoma:About one percent of adult thyroid cancers70%and all of childhood thyroid cancer. It is mostly found in21-40Age female, low malignancy, slower growth, earlier cervical lymph node metastasis, better prognosis.
- 滤foamy carcinoma:About one percent of thyroid cancers15%. Commonly found in50females around the age of 18, with moderate deterioration, rapid progression, and a tendency to invade the vasculature.33%It can metastasize to lung, liver, bone and central nervous system via blood transport, and the prognosis is not as good as that of papillary carcinoma.

- Undifferentiated carcinoma:approximately5%-10%. Mostly found in70highly deteriorating and rapidly progressing around the age of about50%There are cervical lymph node metastases at an early stage, or invasion of the posterior recurrent nerve, trachea or esophagus, and often metastasize to the lungs and bones via blood transport, with a very poor prognosis.
- Medullary carcinoma:occupy only7%, often with a family history. Derived from parafollicular cells (Ccells), secreting large amounts of calcitonin. The degree of deterioration is moderate, lymph node metastasis and hematological metastasis appear earlier, and the prognosis is not as good as that of papillary and follicular carcinoma, but better than that of undifferentiated carcinoma.
symptoms
Papillary carcinoma and follicular carcinoma usually have no obvious symptoms in the early stage. With the progression of the disease, the tumor gradually increases in size, hardness, uneven surface, and the mobility of the mass decreases when swallowing. Undifferentiated carcinoma develops rapidly and invades surrounding tissues. In advanced stage, hoarseness, dyspnea or dysphagia may occur due to the compression of recurrent laryngeal nerve, trachea or esophagus; if the cervical sympathetic ganglion is compressed, it may produce the following symptomsHornersyndrome; if the superficial branch of the cervical plexus is invaded, there may be pain in the ear, occiput and shoulder. There may be cervical lymph node metastasis and distant organ metastasis. Cervical lymph node metastasis occurs earlier in undifferentiated carcinoma. Some patients with inconspicuous thyroid lumps may find metastatic foci first, and should think of the possibility of thyroid cancer when seeking medical treatment.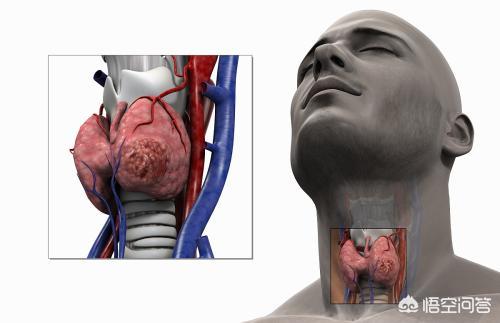
curing
surgical resectionIt is the basic treatment for all types of thyroid cancer (except undifferentiated cancer). Depending on the patient's condition, it is supplemented by endocrine and external radiation therapy.
Welcome to the team of MDs at Tiantan Hospital, Fu Wai Hospital, Institute of Pediatrics, and Peking University Dental Hospital! We wish you good health and a happy life!
I. What is thyroid cancer?
Thyroid cancer is composed of several types of carcinomas with different biological behaviors and different pathological types, mainly including papillary adenocarcinoma, follicular carcinoma, undifferentiated carcinoma and medullary carcinoma. Their age of onset, growth rate, metastatic pathways, and prognosis are significantly different, such as the 10-year survival rate of papillary adenocarcinoma is nearly 90% after surgery, while undifferentiated carcinoma has a very short course and usually survives for only a few months.
Second, how can you tell if you have the disease?
1. Thyroid function tests: mainly thyroid-stimulating hormone (TSH) measurements. high-functioning hot nodules with reduced TSH are less likely to be malignant, so it is more important to treat them for hyperthyroidism. thyroid nodules with a normal or elevated TSH, as well as cold or warm nodules with a reduced TSH should be further evaluated (e.g., by puncture biopsy, etc.).
2. Nuclide scanning: Isotope scanning tests (ECT) with radioactive iodine or technetium are important in determining the functional size of thyroid nodules.
3. Ultrasound: Ultrasound is an important means of detecting thyroid nodules and initially determining whether they are benign or malignant, and it is the criterion for the possibility of fine-needle aspiration biopsy (FNA), and it is also the most cost-effective means of examination. Indications of malignancy under ultrasound include: hypoechoic nodules, microcalcified foci, abundant blood flow signals, unclear borders, nodule height greater than width, solid nodules, and absence of a halo. Some people in China have analyzed and evaluated the nodules in terms of nodule morphology, border, aspect ratio, peripheral halo, internal echogenicity, calcification, and cervical lymph nodes, and compared with postoperative pathological results, statistically concluded that nodule morphology, calcification, and internal echogenicity are more relevant in the benign/malignant differentiation of thyroid nodules, and this aspect of the characteristics can be emphasized (only for papillary carcinoma).
4. Needle aspiration smear cytology: needle aspiration biopsy includes fine needle aspiration biopsy and coarse needle aspiration biopsy, the former is cytology and the latter is histology. For thyroid nodules suspected of malignancy found by ultrasound, this method can be used to make a clear diagnosis.
III. How can it be prevented?
1. Low iodine diet
Follicular thyroid cancer is most common in countries with diets low in iodine. Dietary iodine deficiency may increase the risk of papillary thyroid cancer if there is concurrent exposure to radioactivity.
2. Radiation
Radiation is one of the risk factors for thyroid cancer. Sources of radiation include radiation from medical treatments, leaks from nuclear power plants or nuclear weapons. Having been treated with radiation to the head and neck alone also increases the risk of thyroid cancer. The risk depends on the dose of radiation and age. In general, the higher the dose and the younger the age, the greater the risk will be.
Treating certain childhood cancers (e.g., lymphomas, tumors, neuroblastomas) with radiation therapy also increases the risk. However, cancers that develop as a result of radiation therapy are no more serious than other types of thyroid cancer. x-rays and CT scan imaging also expose your child to radiation, but at much lower doses, so it's not clear how much they increase the risk of thyroid cancer (or other cancers). To be safe, these tests should not be done on your child unless they are very necessary.
Click here for a guide to thyroid self-care.
Thyroid cancer is one of the most common malignant tumors of the thyroid gland, with a higher incidence in women than in men, with the highest incidence in young adult women. Clinically, there are four pathological types of thyroid cancer, namely medullary carcinoma, follicular carcinoma, papillary carcinoma and undifferentiated carcinoma, and the best prognosis is the most common papillary carcinoma. There are many common causes of thyroid cancer, for example, the human body suffers from too much radiation, which deforms the cell nucleus and induces cancer; the intake of certain foods or drugs will interfere with the normal synthesis of thyroid hormones and affect the normal metabolism of the thyroid gland, and the most common cause is the abnormality of iodine intake; and the patients suffering from benign thyroid diseases, such as goiter and hyperthyroidism, are also the common group of people who suffer from thyroid cancer.
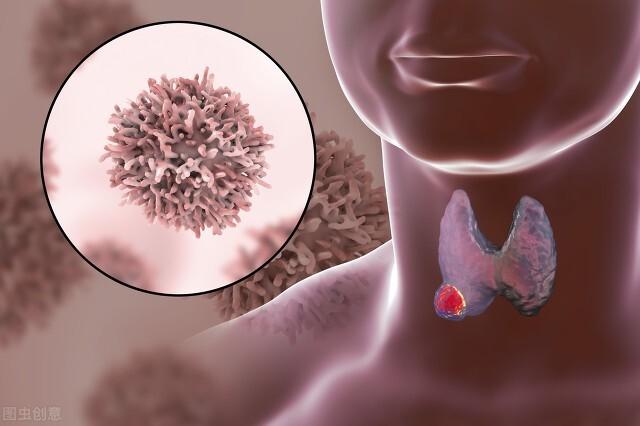
Thyroid cancer is simply the development of cancer in parts of the thyroid gland, mainly papillary, microscopic, medullary, and undifferentiated carcinomas.
Of these thyroid cancers, except for undifferentiated carcinoma, which has a relatively low cure rate, the cure rate is high and the postoperative outcomes are exceptionally good.
So don't worry if you have thyroid cancer, live well and everything will be fine!
Half a month ago, Ms. Li had an operation for thyroid cancer. Yesterday, a few of my colleagues went to visit her, and she is recovering very well, with no discomfort at the moment.
The following is Li's account: 3 months ago, the company organized a physical examination, ultrasound showed thyroid nodules, the border is not fuzzy, at that time did not take it too seriously, check out the nodules of a lot of people, said that it does not matter, but the physical examination center called her and asked her to go for a review, although not too concerned about it, but it is always a matter of concern, and took a weekend to go to the hospital to review the doctor examined, but the doctor recommended that the diagnosis of the puncture.
A few days later, I went to the hospital to pick up the report, the machine showed that it could not be printed, and I thought I was quite unlucky, how could it be my turn that the machine was broken, and I was still in a hurry to go home to be with my child. I went to the front desk to ask for help, the receptionist looked at the machine is not broken, and helped me to make a phone call, said let go directly to the department.
When I got the report, I couldn't describe my feelings, I was scared, worried and thought of all kinds of bad results, and then I cried a lot despite the strange looks from people. After I cried, I thought I had to face the situation, and I took a picture of the report and sent it to my husband, who came over soon and talked to the doctor with me, and finally decided to have the surgery.
The time for the surgery was set, followed by a series of tests, preparation, the surgery was very successful, and the family took good care of me after the surgery, and I recovered relatively well.
Thyroid cancer is also known as "happy cancer" in clinical practice, because after standardized treatment, the 5-year survival rate is as high as more than 95%, and the 20-year survival rate is more than 90%. In general, the prognosis of thyroid cancer is relatively good, and the survival period is longer than that of ordinary cancers.
What is thyroid cancer?
Thyroid cancer is the most common thyroid tumor, and its incidence has grown rapidly over the past two decades, ranking fifth in the incidence of malignant tumors in women. The vast majority of thyroid cancers are slow-growing and rarely fatal, but they should not be ignored because of their lazy metastatic nature, as medullary and undifferentiated carcinomas are among the more critical subtypes, which, although accounting for a relatively low percentage of the cases, can be fatal and also require special attention.
What is the difference between thyroid cancer and thyroid nodules?
Epidemiologic studies have shown that in areas of relatively adequate iodine intake, the prevalence of thyroid nodules by palpation is about 5% in women and 1% in men; ultrasonography detects 19-68% of thyroid nodules. Of the patients with thyroid nodules, 7-15% will develop thyroid cancer.

Thyroid ultrasound is the preferred and mandatory item for thyroid examination. Thyroid cancer, compared with thyroid nodules, is characterized by: 1. irregularly shaped nodules with unclear borders; 2. longitudinal to transversal diameter ratios greater than 1; and 3. scarce or abundant blood flow signals on color Doppler ultrasound.
Thyroid puncture aspiration biopsy is the most commonly used method for preoperative qualitative diagnosis of thyroid cancer, and it is the "gold standard" for confirming the diagnosis. Therefore, those who are suspected of having thyroid cancer can confirm the diagnosis through puncture, and in addition, preoperative diagnosis can reduce the number of unnecessary surgeries.
I am Pharmacist Wang, insisting on spreading knowledge of diseases in simple and easy-to-understand words, and dedicating my own small contribution to a healthy China. If you think my answer is helpful to you, please leave a like! In addition, if you still have related questions, welcome to leave a message, we discuss together!
Thyroid cancer is the most common malignant tumor of thyroid gland, including papillary carcinoma, follicular carcinoma, undifferentiated carcinoma and medullary carcinoma. In the clinic, papillary carcinoma is the most common, and it can be treated by surgery, supplemented with postoperative iodine 131 treatment, endocrine therapy and endocrine therapy, etc.; whereas, follicular carcinoma, undifferentiated carcinoma and medullary carcinoma are more rare, among which, undifferentiated carcinoma has the worst prognosis. Generally, chemotherapy and systemic immune supportive therapy can be chosen to alleviate the condition.
This question and answer are from the site users, does not represent the position of the site, such as infringement, please contact the administrator to delete.