Can prolonged use of antihypertensive drugs harm the kidneys?
Often, when friends inquire about the treatment of hypertension, they ask me whether antihypertensive drugs hurt the kidneys, especially male friends who are afraid to insist on the medication for fear that the antihypertensive drugs hurt the kidneys.
So, do antihypertensive drugs hurt the kidneys?
Let me clarify two concepts for you.
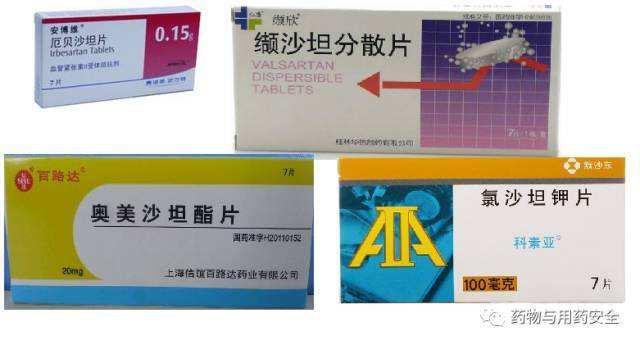
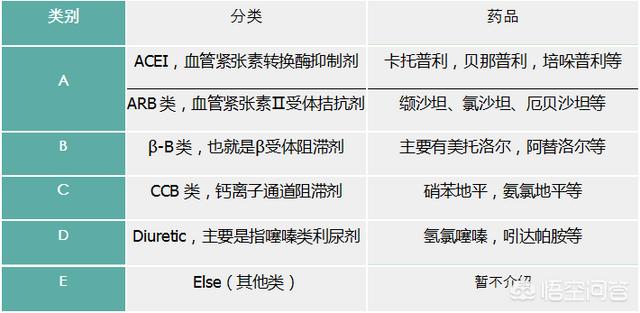
One is the problem of antihypertensive drugs. There are six categories of antihypertensive drugs currently in clinical use: sartans (e.g., Biloxi, Devin), diphenhydramine (e.g., Loxodine), prilosec (e.g., Lodinexin), diuretics (e.g., hydrochlorothiazide), beta-blockers (e.g., bethanechol), and alpha-blockers (e.g., terazosin), with the first four of these categories being the first line of antihypertensive drugs, meaning that they are the preferred drugs to be used. Antihypertensive therapy is given in combination.
The other is the problem of the kidneys. We often say that the kidney includes two elements, one is the modern medicine of the kidney, refers to the organ, which is commonly known as "waist", with excretory and endocrine functions; the other is the traditional medicine of the kidney, refers to certain functions, including sexual function. The common term "injury to the kidneys" actually means damage to sexual function, which is also a concern for many men.
Sartans and Prilosec antihypertensive drugs have the pharmacological effects of lowering blood pressure, lowering urinary protein and delaying renal damage, and are the drugs of choice for the treatment of kidney disease; diphenhydramine antihypertensive drugs have the effect of dilating the renal arteries and lowering blood pressure, and also have a protective effect on the kidneys. These three types of drugs not only do not hurt the kidneys, but also protect the kidneys, and the other three types of drugs have not been found to have a damaging effect on the kidneys.
Most of the male sexual dysfunction (impotence, premature ejaculation, etc.) are functional disorders, which are often referred to as psychological disorders, and only a very small part of them are organic sexual dysfunction. The main cause of male organic sexual dysfunction is atherosclerosis, which leads to erectile dysfunction. And hypertension, high blood pressure, high blood fat, smoking and diabetes are the four major risk factors for atherosclerosis. Control of blood pressure itself is the main means of treatment of atherosclerosis, improve male sexual function, antihypertensive drugs as the "protector" of the kidneys, how can we say that hurt the kidneys?
Long-term high blood pressure causes damage to the heart, brain, kidneys and other major organs of the body, and antihypertensive treatment, even if antihypertensive drugs have a small number of side effects, that is minimal compared to the harm of high blood pressure.
High blood pressure must be controlled up to standard, regular antihypertensive drugs please feel free to use.
 Some hypertensive patients are affected by the traditional ideas of "kidney is the foundation of the innate", "medicine is three times poisonous" and "western medicine hurts the liver and kidney", so they don't take medicine when they suffer from high blood pressure, or they only use some traditional Chinese medicines and refuse to use western medicines. They refuse to use western medicines. However, it is not known that western medicines are effective in lowering blood pressure, and Chinese medicines can only improve the symptoms of hypertension. In the end, the blood pressure rises, unknowingly damage the whole body's large, medium and small blood vessels, damage to the heart, brain, kidney and other organs function, wait until the development of target organ damage and then use the drug, has lost the best time for treatment. So is long-term antihypertensive drugs hurt the kidneys?
Some hypertensive patients are affected by the traditional ideas of "kidney is the foundation of the innate", "medicine is three times poisonous" and "western medicine hurts the liver and kidney", so they don't take medicine when they suffer from high blood pressure, or they only use some traditional Chinese medicines and refuse to use western medicines. They refuse to use western medicines. However, it is not known that western medicines are effective in lowering blood pressure, and Chinese medicines can only improve the symptoms of hypertension. In the end, the blood pressure rises, unknowingly damage the whole body's large, medium and small blood vessels, damage to the heart, brain, kidney and other organs function, wait until the development of target organ damage and then use the drug, has lost the best time for treatment. So is long-term antihypertensive drugs hurt the kidneys?
The commonly used antihypertensive drugs are diuretics (hydrochlorothiazide, indapamide, etc.), diphenhydramine (amlodipine, felodipine, etc.), priligy (enalapril, fosinopril, etc.), sartans (chlosartan, valsartan, etc.), and lorazepam (metoprolol, bisoprolol).
Among these five commonly used antihypertensive drugs, most of the diphenhydramine analogues are metabolized in the liver, e.g., amlodipine is extensively (about 90%) metabolized to inactive metabolites through the liver, the other 10% are excreted in the form of the original drug, and 60% of the metabolites are excreted in the urine, and the pharmacokinetics of amlodipine are unaffected by renal impairment. Therefore patients with renal failure should still be treated with the usual initial dose. This means that patients with renal failure can also take normal doses of amlodipine, i.e. amlodipine does not damage the kidneys.
Metoprolol, another example of a lorazepam, is metabolized primarily in the liver by CYP2D6, and three major metabolites have been identified, none of which have clinically significant beta-blocking effects. The plasma half-life is 3-5 hours. Approximately 5% of metoprolol is excreted renally as a prototype and the remainder is metabolized. Since renal function has no significant effect on metoprolol clearance, no dose adjustment is required in patients with renal impairment. It is evident that metoprolol also has no adverse effect on renal function in patients.
Indapamide in diuretics is metabolized primarily in the liver, producing 19 metabolites. Approximately 70% are excreted renally, of which 7% are in their original form, and 23% are excreted via the gastrointestinal tract. Pharmacokinetic parameters are not altered in renal failure. Only anuria or severe renal insufficiency can induce azotemia.
Prilosec/sartans can reduce renal vascular resistance, improve intraglomerular hypertension, hyperperfusion and hyperfiltration, and improve the selective permeability of glomerular filtration membrane to reduce urinary protein excretion. Clinical studies have confirmed that, in diabetic patients, Prilosec/sartans can prevent the progression of microalbuminuria to macroalbuminuria, effectively reduce urinary albumin excretion, and delay the development of renal lesions.
Prilosec/sartans dilate the glomerular outflow arteries > dilate the glomerular inlet arteries, glomerular filtration pressure decreases, renal function decreases, glomerular filtration rate decreases, and blood creatinine and potassium levels increase. Therefore, in patients with stage 4 or 5 chronic kidney disease, halve the initial dose of prilosec/sartan and monitor closely for changes in potassium and creatinine levels and glomerular filtration rate. Use with caution in patients with creatinine levels ≥ 3 mg/dl.
Although some antihypertensive drugs can elevate blood creatinine levels and diminish renal function. But generally are reversible, after stopping the drug, most can return to normal. Therefore, hypertensive patients should not be afraid of the rat, too worried about the adverse effects of drugs and do not use drugs resulting in damage to the heart, brain, kidney and other organs. As long as the rational application, regular monitoring, both to ensure that the blood pressure standard, but also to prevent the adverse effects of drugs.
Can prolonged use of antihypertensive medication harm the kidneys? This question can be said to be the most frequently asked topic in the field of hypertension. The reason why this question is asked a lot is that it reflects a contradictory psychological state of the majority of hypertensive patients: on the one hand, they are afraid that uncontrolled hypertension will hurt their body; on the other hand, they are afraid that taking antihypertensive drugs will hurt their kidneys. So, how should we recognize this problem? Antihypertensive drugs in the end will not "hurt the kidneys"?
When it comes to the topic of antihypertensive drugs hurt the kidney, in fact, many antihypertensive drugs are not metabolized by the kidneys, many of them are metabolized by the liver, the idea of hurting the kidneys is not necessary. However, on the issue of antihypertensive drugs that hurt the kidneys, we mainly focus on the two types of drugs, prilosec and sartan. Because a lot of scientific information will also tell you, for patients with severe renal insufficiency can not eat Prilosec and Sartan antihypertensive drugs, it can be said that they are not recommended to eat. From this point of view, the general public will think that it is because Prilosec and Sartan antihypertensive drugs have direct damage to the kidneys, so they are not recommended to eat, in fact, the truth is not so.
Generally speaking, no matter what antihypertensive drugs you take, as long as you are able to control your blood pressure smoothly and up to standard, you can play a role in protecting your kidneys. There is no doubt that the kidneys benefit from good blood pressure. Among the various antihypertensive drugs, Prilosec and sartan antihypertensive drugs, in addition to lowering blood pressure to bring about the role of renal protection, additional protection of renal function, reduce proteinuria, and improve the role of insulin resistance. Therefore, Prilosec antihypertensive drugs and sartan-type antihypertensive drugs for most hypertensive patients, as long as there are no contraindications such as bilateral renal artery stenosis, pregnancy, hyperkalemia and other contraindications, can be eaten, and eaten to protect the kidneys.
However, if the blood creatinine of hypertensive patients exceeds 265umol/l, or the glomerular filtration rate is lower than 30, this time you can no longer take Prilosec antihypertensive drugs and sartan antihypertensive drugs. The main reason is not that these two types of drugs will directly damage the kidneys, mainly because these two types of drugs can dilate the glomerular glomerular arteries, resulting in a sustained reduction in renal perfusion, which will add to the originally severely impaired renal function. Therefore, for blood creatinine more than 265umol / l, or glomerular filtration rate of less than 30 hypertensive patients, is not recommended to take Prilosec antihypertensive drugs and sartan antihypertensive drugs.
The above is Dr. Zhang's answer to the question, "Will prolonged use of antihypertensive drugs harm the kidneys?" I hope that my answer will dispel most people's worries, let a few people avoid harm, and let more people benefit from it.

Many drugs are metabolized by the liver and kidneys, but most of the antihypertensive drugs have a relatively small effect on the kidneys. For example, RAS blockers are even good for kidney function, but patients with severe kidney disease need to avoid applying this kind of drugs. Generally speaking, if patients with normal renal function take the commonly used drugs, it should not be a big problem.
In fact, poorly controlled blood pressure will do more harm to the kidneys. If the blood pressure is elevated for a long time, it will damage the blood vessels of the kidneys, which may lead to hypertensive nephropathy or even renal failure in the long run.
Side effects of antihypertensive drugs may occur, but not in everyone.
The best way to avoid kidney damage by high blood pressure is to follow the doctor's instructions to use medication reasonably and keep the blood pressure in the normal range.
Antihypertensive drugs are generally safe for the kidneys as long as they are taken in accordance with medical advice. The side effects of antihypertensive drugs have been well studied by the relevant organizations before the drugs are launched on the market, and these risks can be controlled through regular review and timely adjustment of drugs.
All this to say or, to control the blood pressure in the normal range is the greatest protection of the body, blood pressure control is not good, the body caused by the more serious damage, to sacrifice the end is not a wise move.
If your blood pressure is well controlled and you are not experiencing any adverse effects, it is a good indication that your current medication regimen is very appropriate for your individual situation, and you should not discontinue your medication at will, as this can be dangerous.
Antihypertensive drugs "hurt the kidneys" should be considered from two aspects, one refers to the impact on kidney function, and the other refers to the impact on male sexuality.
I. Impact of hypertension on the kidneys
Chronic hypertension can lead to renal impairment, which usually occurs 10 years after the onset of hypertension. Uncontrolled hypertension will cause glomerulosclerosis, renal unit atrophy, and renal decompensation, and in severe cases, chronic renal failure will develop. Initial symptoms include increased urine output at night with trace protein in the urine, and blood creatinine will slowly increase. Continue to develop into end-stage renal failure, need dialysis treatment. Therefore, hypertensive patients should be actively engaged in antihypertensive treatment, and regular renal function tests.

II. Impact of antihypertensive drugs on renal function
Commonly used antihypertensive drugs are categorized as calcium channel blockers (CCB diphenhydramine class), angiotensin-converting enzyme inhibitors (ACEI prilosec class), angiotensin receptor II blockers (ARB sartans), beta-blockers (lorazepam class), and diuretics. Depending on the pharmacologic action, they have different effects on the kidneys.

1, CCB drugs can dilate small arteries to produce diuretic effect, no effect on renal function.
2, ACEIs are a "double-edged sword", both to protect renal function and cause acute renal failure and hyperkalemia, but as long as the renal perfusion is adequate, ACEIs can slow down the development of chronic kidney disease and kidney injury.
3, ARB drugs can selectively dilate small renal arteries, reduce intraglomerular pressure, there is protection of the kidneys to delay the process of chronic renal insufficiency.
4, Lorazepam will reduce cardiac output, will reduce renal blood perfusion, have a certain impact on renal function. They themselves need to be metabolized by the kidneys, so they should be used with caution in patients with renal insufficiency.
5, diuretics main site of action for the kidneys, long-term application will lead to diuretic dependence, aggravate chronic renal insufficiency. Therefore, when applying diuretics, attention should be paid to checking renal function.

III. Impact of antihypertensive drugs on male functioning
According to a two-year foreign observation of elderly patients using antihypertensive drugs. Diuretics, β-blockers and central antihypertensive drugs (contained in some compound preparations, such as colistin and reserpine, etc.) among antihypertensive drugs can cause erectile dysfunction (ED) in men; while CCBs and ACEIs among antihypertensive drugs have a neutral effect on male function; and ARBs among antihypertensive drugs can improve male function.
The process of erection in men is actually the process of blood engorgement. Any disease that causes congestion can cause erectile dysfunction (ED) in men. The most important cause of ED in elderly patients is atherosclerosis, and among the risk factors for atherosclerosis, high blood pressure is the most dangerous, followed by high blood lipids, high blood sugar and smoking. Therefore, it is not antihypertensive drugs but high blood pressure that harms men's function.

Fourth, how to protect the kidneys of hypertensive patients
To protect the kidneys, patients with high blood pressure should adhere to medication on the basis of a healthy life. Keeping blood pressure within a reasonable range and having regular kidney function checks to prevent damage to the kidneys from high blood pressure is the only way to avoid damage to the kidneys. Regarding male function, hypertensive patients are twice as likely to develop ED compared to those with normal blood pressure. However, it can be improved through increased exercise, healthy diet and weight reduction. A survey showed that 56% of ED patients were improved by adhering to life interventions for two years.

Without a healthy body, there is no happy life. Antihypertensive drugs have positive significance in controlling blood pressure and protecting the function of organs. Therefore, the use of antihypertensive drugs will not "hurt the kidneys". The proper use of medication and a healthy life can better protect the kidney function. If you have any problems with your medication, please contact your doctor or pharmacist.I am Pharmacist Wazi, welcome to follow me and let me be the pharmacist by your side!
Many people with high blood pressure are reluctant to insist on long-term medication to control their blood pressure, and one of their main concerns is - will long-term use of antihypertensive drugs hurt the kidneys? In fact, this is a misunderstanding, although many drugs are metabolized and excreted through the liver and kidneys, but not through the kidney excretion of drugs, will hurt the "kidney".
Correspondingly, if because of the fear of "injury to the kidneys" and antihypertensive drugs to eat and stop, hypertension long-term control is not good, will really hurt the kidneys! Kidneys are one of the target organs of long-term uncontrolled high blood pressure harm, long-term high blood pressure if not controlled, the walls of blood vessels are subjected to greater pressure for a long time, the impact of this pressure also includes the rich blood vessels in the kidneys, long-term high blood pressure is not controlled, the kidneys in the small arteries will also produce sclerosis, and will also affect the kidneys of the renal tubules, the renal mesenchyme, etc., health, high blood pressure nephropathy, is a clinically common class of kidney disease, and the decline in kidney function will also be the kidney, the kidneys will not be able to control high blood pressure. Hypertensive nephropathy is a very common clinical class of kidney disease, and the decline in renal function will lead to the problem of sodium retention, thus further elevating blood pressure, high blood pressure in addition to the renal harm, while the cardiovascular and cerebral vascular harm is even greater, therefore, if you do not control the blood pressure, it will form the damage to the kidneys, and the reduction of renal function will further lead to the elevation of blood pressure, which is really a disgusting cycle, the loss outweighs the gain.
With the continuous progress of drug development, the most commonly used antihypertensive drugs in the clinic now have five major categories, calcium antagonists (such as various types of diphenhydramine), angiotensin-converting enzyme inhibitors (such as various types of prilosec), angiotensin II inhibitors (such as various types of sartan), β-blockers (such as various types of lorazepam), and diuretics, which are commonly used in the control of high blood pressure, and for the different types of hypertensive Patients can reasonably choose these drugs to control blood pressure and keep it within the ideal range.
Do these drugs harm the kidneys? The vast majority of these drugs, taken over a long period of time, do not adversely affect kidney function. In fact, most antihypertensive drugs, such as amlodipine, most of the sartans, and prilosec, do not need to be adjusted in dosage even if there is some problem with kidney function (not due to antihypertensive medication), which is another side of the story that the vast majority of antihypertensive drugs, taken over a long period of time, do not affect renal function. This also shows that the majority of antihypertensive drugs, long-term use, will not affect kidney function.
In addition to not harming even, for the two types of drugs, sartans and Prilosec, because of its role in dilating the renal artery vasculature, but instead have a certain improvement in proteinuria, the role of protecting the kidneys, therefore, for diabetes combined with high blood pressure, micro-proteinuria combined with high blood pressure patients, taking this type of drugs to control the blood pressure, is a very good choice. Chlorosartan in the sartan class of drugs, for patients with high uric acid, there is also a certain promotion of uric acid excretion, the same is also a role in protecting the kidneys. But for these two types of drugs, there is a point to note, that is, patients with bilateral renal artery stenosis problems, should be prohibited.
The claim that antihypertensive drugs harm the kidneys also originates from another claim that some male friends, especially those who are sexually active originally, after taking certain antihypertensive drugs, found that the sexual function has declined, and then thought that it was "harming the kidneys". This is the Chinese medicine theory of "kidney", not the Western medicine said kidney function. So which drugs will affect sexual function? For antihypertensive drugs, clear impact on sexual function of the drug has two categories, one is a diuretic, the other is Lorazepam, long-term use, may affect the male sexual function. But some friends, taking diphenhydramine drugs, and even prilosec drugs, also feel the impact of sexual function, this situation should not be considered first of all the problem of taking medication, from other aspects of the reason to find, strengthen the exercise exercise, promote life conditioning, for theImprovement of ED problemsIt is also very important.
Finally summarize the following, long-term use of antihypertensive drugs will not hurt the kidneys, if the fear of injury to the kidneys, and lead to not dare to take medication, long-term high blood pressure is not controlled, is really "hurt the kidneys"!
Long-term hypertension will cause glomerulosclerosis and affect kidney function, so no matter how, antihypertensive treatment is beneficial to kidneys. However, there are many types of antihypertensive drugs, and there are also differences in the same class of drugs. The effects of different antihypertensive drugs on the kidneys are not comparable, and I will introduce them below:
1. Calcium antagonist: It should be the safest class of antihypertensive drugs at present, without obvious contraindications. These drugs have different effects on renal function because of the different channels of action. Nifedipine, which acts on the L-type channel, may increase the intracapsular pressure in the kidney and increase the urinary protein; amlodipine and felodipine, which act on the L/N-type channel, have less effect on urinary protein, while benidipine, which acts on the L/N/T-type channel at the same time, is thought to reduce urinary protein and protect the kidney.
2. Angiotensin-converting enzyme inhibitors/angiotensin II receptor antagonists (ACEI/ARB class): the rational use of this class of drugs can effectively reduce the renal triad status, which is currently considered the most protective class of drugs for the kidneys. However, improper application of this kind of drugs exceeds the self-regulation ability of the kidneys, but will accelerate the damage to the kidneys, so the following should be avoided during the medication: dehydration (including a large amount of diuresis, vomiting, diarrhea, sweating, etc.); taking painkillers, antipyretics, and so on.
3. Diuretics: A large number of diuretics can cause electrolyte disorders and at the same time lead to insufficient effective perfusion pressure of the kidneys and renal function impairment, especially when combined with ACEI/ARB drugs. In addition, long-term use of diuretics and thiazide diuretics may cause uric acid elevation and thus affect renal function, need to pay attention to monitoring.
4. Several other classes of drugs have no significant effect on renal function.
In conclusion, different antihypertensive drugs have different effects on the kidneys, and only by mastering the correct way of taking the drugs, lowering blood pressure smoothly for a long period of time, and controlling the blood pressure within the effective range can we maximize the protection of the kidneys.
The authoritative interpretation of Pharmaceutical Affairs, unauthorized reproduction, plagiarism will be punished.
Hi everyone, I'm Comic Book Guy and I'm happy to answer your questions!
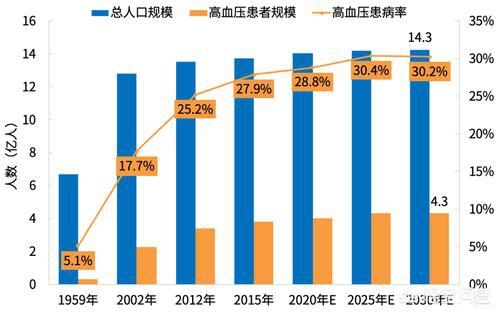
Hypertension, in fact, refers to the pressure of blood flow on the walls of blood vessels, when this pressure is beyond the normal range of blood pressure (120-130/80-90mmHg), it is what we often call hypertension. Nowadays, with the increase of pressure in life, as well as the change of life style, in recent years, the prevalence of hypertension is getting higher and higher, and shows the trend of rejuvenation. For hypertensive patients, if they belong to severe hypertension, they can only take antihypertensive drugs to reduce blood pressure, but the so-called "drugs are three poisons", once a person takes drugs every day, will they have damage to their kidneys? This is also diffuse talk in the background of the private letter and the life of the people asked the most, so, today we will discuss a long time to eat antihypertensive drugs will not hurt the kidney.

Epidemiological characteristics of hypertension
First of all, let's talk about the prevalence of hypertension in China in recent years. According to the data released by the China Center for Disease Control and Prevention, the prevalence of hypertension among residents over 18 years of age in China is 27.8%, of which 29.6% are men and 26.0% are women; in terms of urban and rural distribution, the urban rate is 27.7% and the rural rate is 27.9%, which is not a big difference between the two. For the elderly over 60 years of age who are prone to hypertension, the prevalence rate of hypertension is 58.3%, close to 60%. According to the distribution of blood pressure in China, the prevalence of hypertension decreases in order in the east, center and west regions, with 28.8%, 28.2% and 25.8% respectively. Therefore, the existence of hypertension in different ages, different genders and different regions must be different.
Pharmacologic treatment of hypertension
In clinical practice, in the case of mild hypertension, it may be managed and controlled by dietary control or lifestyle intervention, whereas for patients with moderate to severe hypertension, it may need to be treated by taking blood pressure-lowering drugs. At present, drugs commonly used for lowering blood pressure mainly include 6 categories, which are:Dipyridamole (e.g., Lovenox), Prilosec (e.g., Lotrisin), Sartans (e.g., Biloxi, Devon), Diuretics (e.g., hydrochlorothiazide), Alpha-blockers (e.g., Terazosin), Beta-blockers (e.g., Betalucil)For the control of high blood pressure, of course, you can't just take one medication; sometimes a combination of medications needs to be given in order to achieve good results.
So what is the damage to the kidneys from lowering blood pressure?
Maybe we all have this impression, any kind of drug in the package will have instructions, instructions are based on clinical trials, generally tens of thousands of people's trials, for a variety of drugs to bring the clinical effect, blood pressure control effect, as well as for the kidneys, liver damage, there will be a certain assessment, and at the same time, also in accordance with the appropriate dose to give, so it may be for the kidneys of the damage is negligible, basically in the tolerable range; in addition, for patients with underlying diseases, such as kidney disease will be affected by long-term use of hypertension? In addition, for patients with underlying diseases, such as kidney disease, will long-term use of hypertension have any effect?

First of all, blood pressure in the Puli antihypertensive drugs and sartan antihypertensive drugs, if you take, not only have the role of reducing blood pressure, but also to protect the function of the kidneys, especially patients with kidney disease, can reduce proteinuria to a certain extent, to improve the role of insulin resistance. Therefore, the clinic more recommended Prilosec antihypertensive drugs and sartan antihypertensive drugs for most hypertensive patients to carry out medication to reduce blood pressure.
In addition, for serious kidney disease, such as renal tubulitis, in the case of a certain degree of renal lesions, especially poor glomerular filtration, and even hematuria, it is necessary to pay attention to antihypertensive drugs in the two types of drugs do not try to eat, which will lead to a decrease in blood pressure in the blood vessels, is not conducive to the filtration function of the glomerulus.

In conclusion, antihypertensive drugs are generally not overly toxic for patients with only a single underlying disease of hypertension, and most of the drugs are metabolized in the liver, not in the kidneys, and if drug damage is caused, the first site should be the liver, and the kidneys may only be aggravated on the basis of the medication if there is a lesion in the kidneys themselves. In addition, the management of hypertension is not only about drug control, but also about lifestyle management in order to achieve a better level of blood pressure control.
You mean "for a long time" as in a long time, right? Do you think eating for a long time will make you old? In the long run, people are in a process of "dying" and no one can escape it.
We all know that drugs are three poisons, high blood pressure patients need to take medication for life to smooth control of blood pressure, so that blood pressure tends to a stable state, so that it will be relatively safe. If you have high blood pressure, in order not to hurt the kidneys choose not to take medication, perhaps do not know the day on the sudden illness "dead", the risk factor is too great, the safety of life there is a great potential danger and uncertainty. That's why you need to take blood pressure medication for a long time. Compared to "kidney damage", you think the value of life and organs affected by a little which is more important?
Don't say long-term antihypertensive medication, any medication you take will affect your liver and kidneys to some degree, including Chinese medicine.Sometimes, when faced with a disease, you have to learn to weigh the pros and cons of your medication to get the best out of it.The fact is that it is not always certain drugs that hurt the kidneys. In fact, injury to the kidneys is not necessarily certain drugs, life mentality, environment and way of life are also very important factors, if you follow the doctor's instructions in the safe range of medication, antihypertensive drugs on the body's damage is still controllable.
My father has been suffering from high blood pressure for more than 20 years, and he is hospitalized several times a year. He sometimes does not listen to the doctor, in order to let the disease get well quickly and completely "get rid of" the psychological burden of long-term antihypertensive drugs, sometimes they will take additional antihypertensive drugs, the results really led to kidney damage, the last six months, ankle swelling, high uric acid, urinary protein, but after the treatment, strictly comply with the doctor's instructions with antihypertensive drugs, these symptoms gradually basically disappeared, because the kidneys are the most afraid of indiscriminate use of drugs and overloaded. Gradually basically disappeared, because the kidneys are afraid of indiscriminate use of drugs and overwhelmed. 84-year-old father himself knows, these years, if not long-term adherence to take antihypertensive drugs, he may not even live so long.
In short, friends with high blood pressure, must not take the initiative not to use or indiscriminate use of drugs, that is very dangerous. As long as you follow the doctor to prescribe a safe dose, usually have a good lifestyle and habits, pay attention to often go to the hospital for medical checkups, with the disease to extend the year is no problem, and if you are bent on "bent on", it is not good to say that will increase the risk of sudden illnesses and endangered life.

Image Source Web.
Dr. Duan Q&A Online 🍀Chat about antihypertensive drugs and kidney injury 🍀
In the eyes of everyone, "injury to the kidneys" refers to erectile dysfunction (ED), which affects gay men; while in the eyes of doctors, "injury to the kidneys" is impaired renal function, mainly in the form of oedema, urination and other manifestations. So, in the end, antihypertensive drugs are "to protect the kidney" or "hurt the kidney", let's take a look together.
First, the urgency and importance of antihypertensive treatment was clarified:
(1) China is known to have a large population base of hypertensive patients, according to statistics, there have been as many as 270 million;
(2) As a common disease, hypertension is prone to cause damage to target organs such as the heart, brain, and kidneys;
Therefore, for hypertensive patients, long-term antihypertensive drugs must be taken to reduce target organ damage and minimize complications, so rational antihypertensive treatment is mandatory to implement!
What doctors call "kidney damage":
The kidney is an important organ to regulate blood pressure, hypertension is not effectively treated, it is very easy to cause renal arteriolar sclerosis, renal tubular atrophy and renal interstitial fibrosis, clinical development of renal insufficiency, there are changes in the amount of urine and proteinuria, this is because of hypertension caused by the renal structure and function of the lesions, we call hypertensive nephropathy, so the antihypertensive treatment instead of having a Therefore, antihypertensive treatment has the effect of "preserving the kidney"!
② Some drugs act on the kidneys and are metabolized by the kidneys, so when bilateral renal artery stenosis exists, it is forbidden to use Prilosec and sartans;
(iii) For those who have diabetic nephropathy, the recommended antihypertensive drugs are Prilosec and sartans, but when used in large quantities over a long period of time, it is again necessary to pay attention to the detection of renal function.
"Kidney damage" in everyone's eyes.
(1) Some antihypertensive drugs, including thiazide diuretics, cotrimoxazole, and the central antihypertensive drug colestipol, do have the potential to cause erectile dysfunction (ED), but these antihypertensive drugs are gradually being used less in the clinic because of their poor antihypertensive effect and high side effects;
(2) Some patients taking calcium antagonists (diphenhydramine) as well as ACEIs (prilosec) have also been reported to cause ED, and when this occurs, it is generally recommended to change antihypertensive drug therapy;
(3) Not only does it have no ED effect on ARBs (sartans), it also has a favorable effect, so it can be called the "best of both worlds".
How to protect our kidneys.
(1) Ensure enough water every day to ensure the excretion of metabolic wastes from the body on the one hand; and avoid urinary tract infections on the other;
(2) Adequate rest and nutrition, which ensures normal immunity of the body and avoids external aggression on various organs such as the kidneys;
(3) Moderate exercise, on the one hand, assists the kidneys in excretion through the skin and, on the other hand, improves the body's functioning and avoids damage to the kidneys;
(4) A low-salt, low-fat diet reduces the work compound of the kidneys;
(5) Actively treating the primary disease, especially controlling blood pressure and blood sugar, to reduce kidney damage;
(6) Avoid drugs with kidney damage, such as gentamicin and sulfasalazine;
(7) Stop smoking, limit alcohol, lose fat and weight, not just for your kidneys, but for your overall health.
special attention
(1) When ED does occur from taking certain antihypertensive drugs, you may consider changing the antihypertensive drug under the supervision of your doctor;
(2) Antihypertensive drug therapy has a clear renoprotective effect and can minimize target organ damage;
(3) Only a healthy body is qualified to attach everything on top of that, so weigh your treatment correctly and don't lose out on small things.
(4) Recognize your kidneys correctly; they are more about helping you excrete waste than they are about boosting your virility.
👇Follow Dr. Duan for health and wellness👇.
This question and answer are from the site users, does not represent the position of the site, such as infringement, please contact the administrator to delete.