What happens when a patient with new crown pneumonia is cured and then positive on retest?
The question is timely, and this issue can be said to be a recent hot topic of interest.
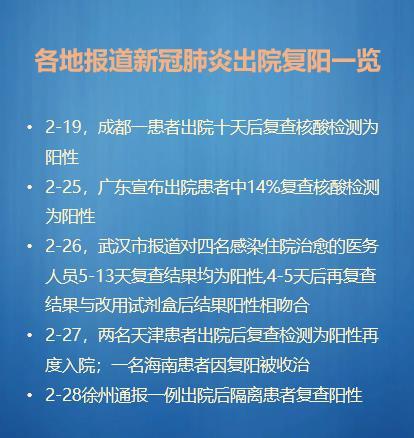
We know that as the general trend of the epidemic improves, most of the new coronary lung patients who have recovered and been discharged from hospitals after careful treatment are negative for nucleic acids. This has allowed the nation to finally see the light of victory. But recently the media from time to time out of patients discharged from the hospital and 're-positive' news appeared, what is this all about? The following is my authoritative media collated from the recent 're-positive' cases:
As seen from the above cases, these re-positive is a number of provinces and cities occurred in sporadic 'cases', can not represent the whole epidemic turn for the better in the general direction, the fundamentals are the overall downward trend do not doubt. To quote Prof. Zhong Nanshan said: as long as the body appeared antibodies, generally these patients will not be infected again, do not say that once found that there is a remnant that re-infection. As for the intestinal feces there are remnants of whether it will be passed on to others, but also need to be observed.
So what are some of the reasons why the virus is causing these patients to go back to positive? First of all, we know that the new coronavirus is a newly discovered virus, human understanding of it is still in the initial stage, even its starting place of origin is under debate. The State Council's Joint Prevention and Control Mechanism's answer at the press conference and the authoritative experts' interpretation, as far as the means of detection is concerned, may exist by the following reasons:
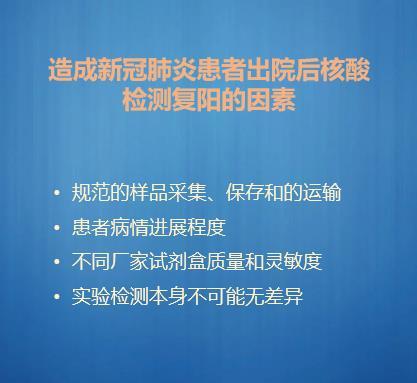
Take for example the sample collection in the first specification: which factor does not affect the quality of the swab collection, from the operator's different maneuvers and proficiency in their application, to the timing of the collection site, to the patient's cooperation? The collected virus specimen must be delivered within the specified effective time and temperature, otherwise the virus will be inactivated. Therefore, under the existing experimental conditions where there are differences in human and material resources around the world, and before the development of a unified post-discharge collection program and the implementation of standards, it is expected that the detection of different results. The above is the reason from the detection means.
Secondly, in the new crown pneumonia re-positive people themselves, after a period of time to experience the destruction of the virus, the body already has immunity, this immunity will last in the body for a period of time. But the virus will not disappear all of a sudden and remain, the time to clear the virus also varies from person to person, it makes sense that there will be re-positive. It is prudent to observe whether the recovered patients will be infected twice or pass on the virus to others. The current practice of allowing recovered patients to be isolated at home for 14 days and to be re-examined or hospitalized if they are found to be re-positive is not only a move to protect the patients but also a responsible one for the public.

In summary, a small number of patients with new coronary pulmonary reactivation do exist, and there is no information on secondary infection or transmission to others; whether they will be positive for life and re-infect themselves, and whether they can cause transmission in the population, need to be followed up with observational studies, but it suggests that we should put forward higher requirements for the discharge criteria of the current cured discharged patients, the period of observation, the criteria for discontinuing isolation, and the continuous patient management. The study is still to be followed up and observed.
Recently, many places have reported cases of "re-testing" of patients with new coronary pneumonia after cure. In Guangdong, 14% of patients discharged from hospitals were initially reported to be positive. So far, many countries such as Japan, South Korea, Canada and the United States have also reported cases of "re-positive" after cure. Many people are concerned about what to do if these "re-positive" cases spread again.
Why is there a "re-positive" phenomenon after cure?
1. Errors in negative results at hospital dischargeNucleic acid tests can be "false-negative". Nucleic acid tests can be "false-negative". Zhao Jianping, director of the Department of Respiratory and Critical Care Medicine at Wuhan Tongji Hospital, said in an interview with China News Weekly, "False negatives may be affected by the sampling technique, the intermittent detoxification of the disease itself, and other factors". In other words, false negatives are related to a variety of factors such as the techniques of our sampling personnel, differences in the kits, and the existence of intermittent detoxification of the virus itself. The positive rate of nucleic acid testing is only about 30% to 50%. IfThe patient's temperature had returned to normal for more than 3 days, his respiratory symptoms had improved significantly, and his repeat chest CT was significantly improved.According to our current discharge criteria, two consecutive respiratory nucleic acid tests at 24-hour intervals are negative before discharge. Although this can reduce the error brought about by the personnel technology and kits, but if there is a phenomenon of intermittent detoxification of the virus, just before the discharge of a small amount of toxicity test negative, and after the discharge of the toxicity and increase, that is, the virus has not yet been completely cleared, then the phenomenon of "repositive positivity" is likely to occur.

2. Possible remnants of a virusAcademician Zhong Nanshan explained at a briefing on the Guangzhou outbreak on February 27 that patients who test positive after being discharged from the hospital may be fecal and intestinal remnants of the virus. That said, it is also possible that a positive retest could be only a residual nucleic acid fragment of the virus. Some patients may test negative on a respiratory specimen but positive on an anal swab. Different people may react differently to the virus, so a negative respiratory specimen alone may not be accurate. Shanghai patients in the discharge, not only to meet the latest version (sixth edition) of the diagnosis and treatment guidelines of the discharge criteria, but also to test the anal swab (fecal) nucleic acid is negative. There have been no reports of patients being discharged from the hospital in Shanghai who have been "re-positive".
But nowAlthough there are many patients who have been discharged from the hospital with "re-positive" results, there has been no evidence of transmission from "retested" patients. There are still many unknowns about this newly discovered virus that need to be explored.
Welcome to like, forward, leave a message, I am physician Yang Hao, focusing on common diseases, multiple diseases diagnosis and treatment, chronic disease management, health science. If you want to know more about medical knowledge, welcome to pay attention to this headline!
There are currently a number of patientsIt was positive again when it was retested after being cured. For example, on February 19, a patient with new coronary pneumonia in Chengdu, Sichuan Province, who went home to quarantine after being cured was retested positive for nucleic acid on the 10th day of his home quarantine, and the relevant organizations have successively picked up the family and the patient.
而14% of patients discharged from hospitals in Guangdong showed "re-positive".A few days ago, when Guangzhou City conducted a follow-up visit to patients who had been cured and discharged from the hospital, it was found that 13 (14%) discharged patients tested positive for nucleic acids, which aroused public concern.
Is a positive re-test after discharge a re-infection?
Can I infect other people with a re-positive?
In fact, under normal circumstances, patients who are discharged from the hospital with a positive nucleic acid test are not usually referred to as "re-infected", but rather there may be patients such asVirus clearance from the body is delayed in older patients. So retesting is still positive, not relapse and reinfection, which are different concepts.
Patients discharged from hospitals cured of SARS were once closely followed and found to beOn CT examination one year after discharge, lung function was essentially normalized.In contrast, patients with new crown pneumonia recovered similarly to SARS patients after discharge from the hospital, with no difference in recovery.
He also suggested that since discharged patients had different physical conditions, patients were advised to be more sedentary than strenuous activities during the period of isolation and recovery from hospitalization.

New Crown Pneumonia is a new infectious disease and we are constantly recognizing it. Pneumonia is a disease with a long incubation period, and some elderly people or people in poor health have a poorer recovery from pneumonia, and we have observed a similar situation with C.N.C. pneumonia.A large proportion of cases of re-positive is inflammation in the process of absorption, not clinical healing, so produce intermittent detoxification phenomenon. But this judgment is still in the scientific evidence .
From microbial properties, if a person is infected with the virus they will produce antibodies. We have found that in young gently ill people, antibodies are produced within two weeks, so the risk of transmission is low, but some elderly people who have a long recovery time and are constantly detoxifying may be a source of infection.
This question and answer are from the site users, does not represent the position of the site, such as infringement, please contact the administrator to delete.