What is essential hypertension?
Primary hypertension is a disease that involves genetically related genes, such as obesity, age, loss of elasticity of the arterial wall due to aging and degeneration, sympathetic nerve excitability, carotid artery pressure receptor sensitivity, renin-angiotensin RAS system activity, salt sensitivity, and so on, and there are many other causes that are still not clear and will never be understood. Anyone who has a systolic blood pressure greater than 140mmHg, a diastolic blood pressure greater than 90mmHg, or one of the two on three different days, at the same time, in the same state, and who excludes secondary hypertension, is called a primary hypertensive.
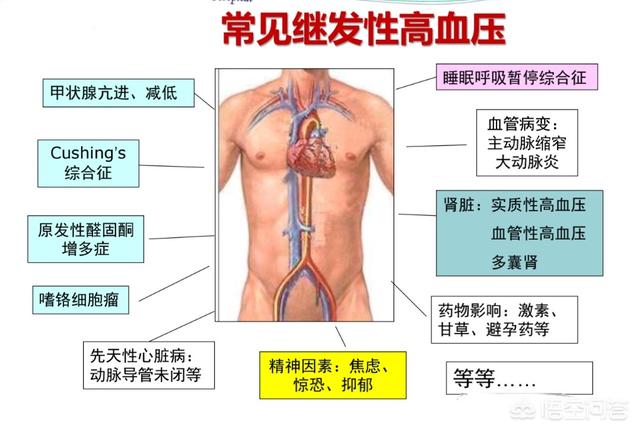
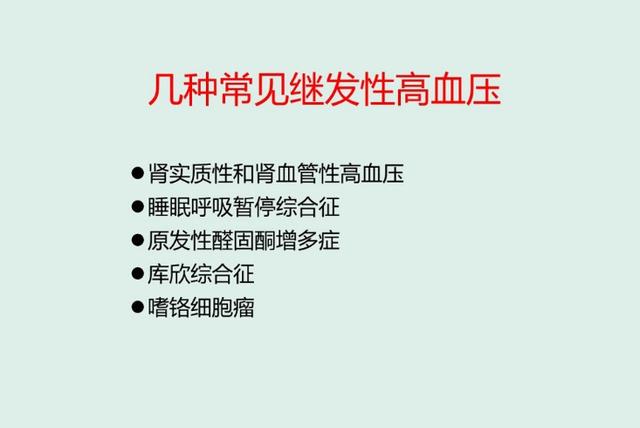
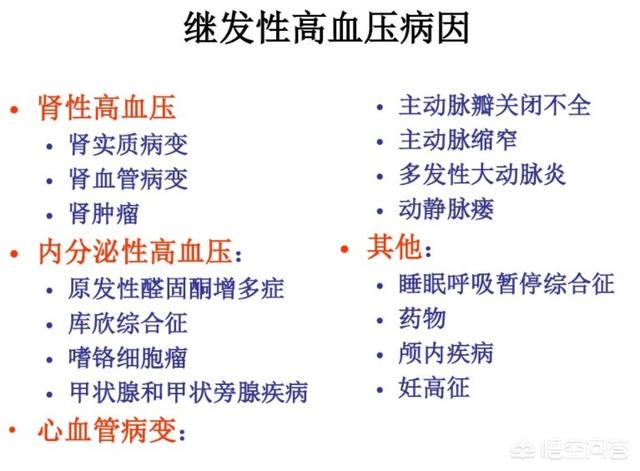
The so-called secondary hypertension refers to hypertension produced by other diseases of the body, such as: renal hypertension (various acute and chronic nephritis, renal arteriosclerosis and stenosis, diabetic glomerulonephritis, etc.), primary or secondary aldosteronism (primary mainly due to adrenocortical tumors, hyperplasia, etc.).Secondary aldosteronism is caused by excessive aldosterone secretion from the adrenal gland due to diseases other than adrenal gland, such as cirrhosis, congestive heart failure, nephrotic syndrome, renal hypertension, etc.) manifested by hypertension and low blood potassium abdominal distension and muscle weakness, pheochromocytoma, and Kirchhoff's syndrome caused by too much glucocorticoid application for too long.
Once diagnosed with primary hypertension one may be on antihypertensive medication for a long time or even for life to reduce the risk of death and disability from heart, brain, kidney and macrovascular disease, although it must be emphasized that hypertension is asymptomatic or no one would ever have a stroke. Questions are often asked about what the precursors are, and more than a few trippers will harp on what turns out to be misleading or scaring readers. Some people will say I dizziness, headache, head and neck stiffness discomfort when the blood pressure is high, that is your recent low head work pressure is too large, too long, of course, will cause blood pressure rise at the same time to produce muscle tension dizziness and headache symptoms, one thing can be sure that not every uncomfortable head measurement of blood pressure is high, of course, high blood pressure does not necessarily have the head of the symptom, which explains the problem. In order to early prevention of early primary hypertension lifelong medication is recommended to pay attention to the following two points:
1. If people with high blood pressure due to significant weight gain in the past two years, if they are determined to strictly control their mouths, manage their hunger and increase their exercise (drinking only water after exercise) so that the excess fat is converted into glycogen for the energy needed for life activities, living and exercise, they will not suffer from gastric problems, and their hunger will not spoil their bodies, but rather they will be starved to a lesser degree, which will reduce the capacity of their stomachs. Good can make the weight loss of 15-20 pounds or more most of the blood pressure will return to normal, and this good mode of life to continue to live a decade, twenty years.
2. A lot of the same factors can affect the fluctuation of blood pressure, such as tension, stress, fear, insomnia, talk too much, emotional factors, etc., and blood pressure measurement tends to be only once, just talked about the human carotid artery pressure receptor sensitivity factors. Therefore, in the diagnosis of hypertension treatment should be done before a 24-hour dynamic blood pressure is very necessary, to confirm the presence of hypertension, the extent of the disease, how to use medication are of great significance. In the past, only emphasize the different three days, etc. because the dynamic blood pressure device has not yet been invented, in the future, not only for diagnosis, treatment, efficacy is one of the best means of inspection and monitoring, should be said to be the gold standard for diagnosis of hypertension. Remember that hypertension is a completely controllable and even reversible disease, hypertension is asymptomatic (except hypertensive encephalopathy), but can damage a variety of important organs of the invisible killer, ignoring it is not only bad luck you and your family.
2018.12.29
What is essential hypertension? This is a good question, and I guess the person who asked this question must have dabbled in introductions related to hypertension. That's why they can say such a specialized name. Today, Dr. Zhang will explain this question to you, and I hope that my explanation can help you.

In fact, all hypertensive patients can be roughly divided into two categories, one is called "primary hypertension" and the other is called "secondary hypertension". Secondary hypertension is generally said to be the patient's high blood pressure secondary to a disease, for example, some patients with high blood pressure secondary to primary aldosteronism this disease, then this disease although manifested as high blood pressure, but in fact it is a kind of secondary hypertension.
However, it should be specifically noted that these conditions only make up a minority of all hypertensive patients. More hypertensive patients actually have primary hypertension, which means that their high blood pressure is not brought about by a particular disease, but by a combination of reasons. For example, long-term high salt diet, lack of exercise, obesity, staying up late, mental anxiety and tension, etc., plus some people have a genetic predisposition to high blood pressure, in these unhealthy factors under the long-term role, some people slowly occur high blood pressure. This high blood pressure at this time in many cases is what we call primary hypertension, this high blood pressure is not brought about by a particular disease, but a variety of risk factors.

In fact, more than 90% of the many hypertensive patients are primary hypertension, and the number of hypertensive patients in China has reached 245 million or even more. This general background reminds us to pay special attention to improving our lifestyles to minimize the occurrence and development of primary hypertension. Improve lifestyle at the same time, many people also need to be under the guidance of a professional doctor for professional treatment, such as the use of antihypertensive drugs to reduce blood pressure. And each person needs to be treated individually, rather than one treatment program for all.
The above is Dr. Zhang's interpretation of primary hypertension, I hope that after reading it you can understand what is primary hypertension, what is secondary hypertension, I hope to be able to help more people.

People find out that they have high blood pressure, try every possible way to find the cause and get rid of it, and stop using antihypertensive drugs, do not monitor their blood pressure, thinking that their high blood pressure is intermittent, not realizing that their blood pressure is high again, and suffering from complications, and in some cases, even dangerous!
Primary hypertension theoretically refers to the difficulty of determining a clear cause, there is no root treatment, most patients (accounting for more than 90% of hypertension) need to take long-term antihypertensive drug treatment. The current hypertension prevention and treatment guidelines do not recommend devices for the treatment of hypertension, these claims are not based on science, is irresponsible and false propaganda.



Primary hypertension is relative to secondary hypertension.
secondary hypertension, is an increase in blood pressure caused by some identified disease or etiology.
Common causes of secondary hypertension are listed below:
Secondary hypertension can often be seen in younger patients, with mostly moderately to severely elevated blood pressure, poor antihypertensive medication even in combination, or blood pressure that fluctuates easily, making acute and malignant hypertension more likely to occur.
Primary hypertension, on the other hand, is high blood pressure for which no clear cause has been found, and its occurrence is generally believed to be related to heredity and the influence of acquired environmental factors. Its primary treatment is controlled by diet, exercise, weight loss and medication.
The conventional wisdom is that secondary hypertension accounts for only 5% of all hypertension, but as diagnostic techniques become more advanced, more patients with secondary hypertension are now being identified. Many experts believe that secondary hypertension may account for well over 5-10% of all hypertension.
If secondary hypertension is treated as primary hypertension, there is a risk of time-consuming, costly and ineffective treatment.
So it is recommended for the following types of hypertensive patients:
hypertensive patients with no family history of
Comparatively young patients with hypertension or new-onset hypertension greater than 55 years of age.
patients with moderately to severely elevated blood pressure.
patients who are not satisfactorily treated with combinations of multiple antihypertensive agents.
Patients with elevated blood pressure accompanied by limb paralysis, weakness, or hypokalemia.
patients with acute and malignant hypertension.
patients with a history of proteinuria or renal disease.
Those who snore and have apnea at night
Hypertensive patients with these conditions should always go to a higher level of care and have a screening for secondary hypertension.
focusDr. Cheng's 100, learn more about common and multiple diseases.
Liking and retweeting so that more people can learn are good habits oh!
Primary hypertension, or hypertension, is a clinical syndrome characterized by an increase in arterial pressure in the body circulation with no known cause.
[Diagnosis]
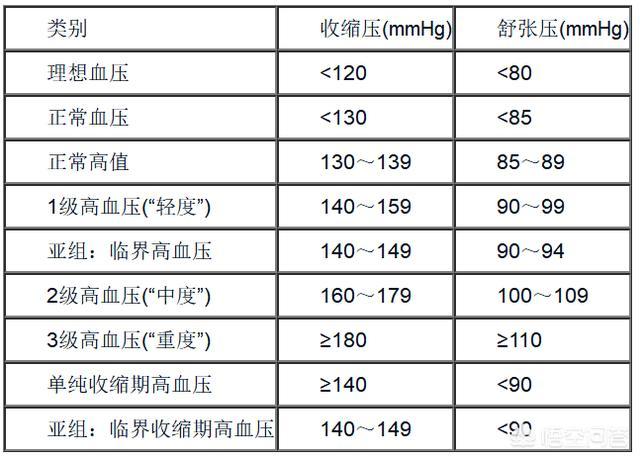
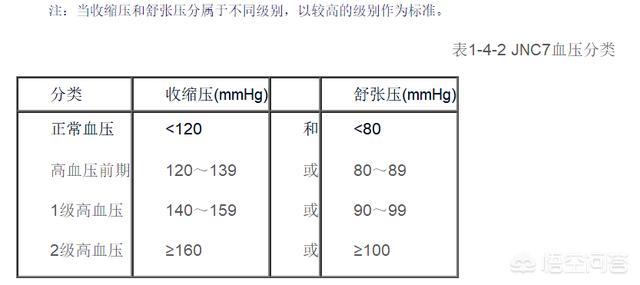
Hypertension is defined as systolic blood pressure ≥ 140 mmHg and diastolic blood pressure ≥ 90 mmHg. The international standardized classification criteria or JNC classification criteria are used to classify hypertension (see Table 1-4-1, 1-4-2). Hypertension is classified according to the International Standard Classification or the JNC classification (see Tables 1-4-1 and 1-4-2).
(Elevated blood pressure must be diagnosed by the average of two or more measurements taken on non-simultaneous days without the use of antihypertensive medication.
To measure blood pressure with the cuff method, the correct method is: the lower edge of the cuff is 2-3 cm from the transverse line of the elbow, the membrane of the stethoscope or the body piece is at the same level as the mid-axillary line, and the two eyes look at the plane of the mercury column. Take two measurements in the same way, with a 1-minute interval, and take the average value.
(iii) Hypertension risk stratification
(1) Risk factors: smoking, age >60 years, male or postmenopausal women, hyperlipidemia, diabetes mellitus, family history of cardiovascular disease (age of onset, <65 years for women, <60 years for men).
Table 1-4-1 Blood Pressure Level Definitions and Classifications (WHO/ISH)
(2) organ damage: ① cardiovascular: left ventricular hypertrophy, angina pectoris, myocardial infarction, heart failure, history of coronary artery bypass surgery; ② cerebrovascular: cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage, transient ischemic attack; ③ kidney damage: proteinuria, serum creatinine increase; ④ retinopathy: four levels. Grade Ⅰ: retinal artery thinning, reflective enhancement; Grade Ⅱ: retinal artery narrowing, arteriovenous cross-pressure; Grade Ⅲ: on the basis of the above, there is fundus hemorrhage, cotton-wool or flame-like exudation; Grade Ⅳ: on the basis of the above, there is optic papillae edema, which is meaningful if it is greater than or equal to Grade Ⅲ or above.
(3) Risk stratification: There are four levels. (1) Low risk: hypertension grade I without risk factors; (2) Medium risk: hypertension grade I with 1-2 risk factors or hypertension grade 2 with or without no more than 2 risk factors; (3) High risk: hypertension grade 1-2 with at least 3 risk factors; (4) Extremely high risk: hypertension grade 3 or grade 1-2 with target organ damage.
(D) Clinical manifestations Hypertension has an insidious onset, progresses slowly, and is asymptomatic in the early stage. Some patients may have headache, dizziness, tinnitus, palpitation, fatigue, and poor sleep, which are not specific and therefore not easy to be detected in the early stage, and are sometimes detected in physical examination. In the ten or several decades after onset of the disease, it will accumulate in the target organs, and then it has already progressed to the serious degree.
In patients with renal damage, the identification of renal hypertension is clinically difficult, but the degree of anemia, especially changes in the fundus of the eye, is of some value, e.g., in patients with chronic nephritis, the fundus of the eye is often pale.
In a few patients, the onset of the disease is acute and the hypertension is critical.
(1) Malignant hypertension: acute onset, rapid progression, sustained elevation of blood pressure, diastolic blood pressure ≥ 130mmHg, headache, blurred vision, hemorrhagic foci in the fundus of the eye, optic papillae edema, significant renal impairment, persistent proteinuria, hematuria, tubular urine, accompanied by renal insufficiency, or even uremia, stroke or heart failure. The characteristic pathological change is fibrinoid necrosis of small renal arteries.
(2) Hypertensive crisis: In the slow course of the disease, the blood pressure rises suddenly and significantly, manifested by headache, nausea, vomiting, irritability, chest tightness, shortness of breath, blurred vision, and even acute left heart failure and hypertensive encephalopathy, the rise in blood pressure is mainly systolic blood pressure, which is caused by the rise in peripheral vascular resistance, and the sympathetic nerve activity rises at this time, with a high concentration of catecholamines in the blood.
(3) Hypertensive encephalopathy: the patient's cerebral blood circulation is impaired, leading to cerebral edema, which increases intracranial pressure and manifests itself in severe headache, nausea, vomiting, trance, confusion, and even convulsions and coma.
(4) Severe systolic hypertension: it is more likely to occur in the elderly or hemodialysis patients, and the blood pressure is mainly elevated in systolic blood pressure, while the diastolic blood pressure is not obvious, and the difference in pulse pressure is large, which indicates that the vascular compliance is poor, and it is easy to be complicated by stroke, acute left heart failure, myocardial infarction, and renal insufficiency, and the fluctuation of the blood pressure is large within one day.
[Treatment]
(i) Non-pharmacological treatment
(1) Reasonable diet, sodium restriction, daily salt intake of no more than 6g, low-fat diet, more vegetables, fruits and other foods rich in vitamins.
(2) Quit smoking and drinking, especially liquor.
(3) Weight loss, moderate exercise, such as walking, brisk walking, do not advocate long-distance running and other strenuous exercise.
(4) Qigong exercise.
(5) Maintain a healthy mind, avoid mental stress and mental injury, high blood pressure in patients with schizophrenia has been reported in cases where the blood pressure dropped after taking anti-schizophrenic drugs, everything should be calm and peaceful, and the mind and spirit should be at ease. Sleeping time should be adequate.
(There are dozens of antihypertensive drugs and new drugs are still being developed, but from the aspect of mechanism of action, there are mainly the following categories: diuretics, β-blockers, calcium antagonists, angiotensin-converting enzyme inhibitors (ACEI), α-blockers, direct vasodilators, angiotensin Ⅱ receptor blockers, peripheral sympathetic nervous system inhibitors, central sympathetic nervous system inhibitors, etc. The first five categories of drugs are recommended by WHO experts as the first-line antihypertensive agents. The first five types of drugs are the first-line antihypertensive drugs recommended by WHO experts.
1. Types of antihypertensive drugs
(1) Diuretics: reduce extracellular fluid and decrease cardiac output, especially for volume-dependent hypertension. The effect is mild, and the efficacy of the drug reaches its peak in 2-3 weeks. Since it can reduce the incidence of cardiovascular events and death rate caused by hypertension, and reverse left ventricular hypertrophy, it is preferred and is used as the basic drug for combined use of antihypertensive drugs, and it should be promoted in the elderly or systolic hypertension or in combination with left heart failure. Thiazide: 12.5-25mg of dihydroclonazepam tablets, 1-3 times/d, increasing the dose is not proportional to the efficacy. Long-term application can lead to a decrease in blood potassium, sodium, blood glucose, blood lipids, blood uric acid rise. ② tabular diuretics: chronic renal failure patients should choose tachycardia, and thiazide is ineffective. The dose of 20-100mg, 1-3 times / d, severe cases of intravenous injection, 40-100mg / d. Excessive application will cause hypotension and low potassium. Hepatitis patients are easy to induce hepatic coma and muscle relaxation, hypogonadism, increased blood uric acid, platelet reduction. Potassium-preserving diuretics: 20-40mg, 3 times/d, 50-100mg of amphotericin, should not be used in combination with ACEI because of elevation of potassium in blood, and is prohibited in patients with chronic renal insufficiency. Gynecomastia, decreased libido, impotence may occur in men, menstrual irregularities, dysmenorrhea, hirsutism, voice coarsening in women, which may disappear on its own after stopping the drug. Indapamide: 2.5-5mg, 1-2 times/d, both diuretic and vasodilator, seldom cause hypokalemia.
(2) β-blocker: ① first generation β-blocker: such as propranolol (cardioplegia), 10 ~ 20mg, 1 ~ 3 times / d, for non-specific blockers. That is, to β1, β2 are blocked, the bronchial smooth muscle β2 receptor blockade, so it is easy to cause bronchospasm, chronic bronchitis patients prohibited. ② The second generation of β-blockers: such as betaxolol, 6.25-50mg, 1-3 times / d, the selectivity of β1 receptor is higher than the first generation. Third-generation β-blockers: such as carvedilol, 12.5-25mg, once / d, both β1-specific blocking function, but also a variety of additional functions, such as α1-receptor blockade, β2-receptor excitability, calcium ion blockade, and some have an intrinsic sympathomimetic activity, such as esmolol, 100-200mg, once / d, but also does not affect lipid metabolism.
(3) Calcium antagonists: ① first-generation calcium antagonists: nifedipine (cardioplegia) 10-20mg, 3 times / d, phenyl dihydropyridine, vascular selectivity is higher than the heart. ② the second generation of dihydropyridines: nitrendipine, felodipine, nisoldipine, nicardipine, amlodipine, etc., 5 to 10 mg, 1 time / d, rapid and stable antihypertensive effect, especially for the elderly systolic hypertension, but it will cause accelerated heart rate, redness, headache, swelling of the lower limbs.
(4) ACEI: It is especially suitable for renin-dependent hypertension, but it is prone to hyperkalemia and cough, and should be started with a small dose and gradually increased to reach the effective therapeutic dose. This drug is classified by JNC7 as a strong indication for 6 conditions (heart failure, post myocardial infarction, high risk factors for coronary heart disease, diabetes mellitus, chronic kidney disease and prevention of recurrent stroke). (1) Mercapto or sulfur group: the first generation of ACEI includes captopril, which is excreted through the kidneys, 12.5-50mg, 3 times/d. It is forbidden to be used in patients with renal artery stenosis, pregnancy, and hyperkalemia. ② carboxylic acid-containing class: second-generation ACEI products such as enalapril, 2.5-20mg, 1 time / d, renal excretion, benazepril (Lodine) 5-40mg, 1 time / d, through the liver, renal excretion, i.e., the "dual-channel" excretion, so it's safer. (iii) Containing hypophosphites: Fopril (Mono) is a third-generation ACEI product, 10-40mg, 1 time/d, also dual-channel excretion.
(5) α-blockers: ① quinazoline: prazosin 1 ~ 2mg, 3 times / d, terazosin (Gautreaux) can be the treatment of prostate hypertrophy, the beginning of the oral 1 time not more than 1mg and then gradually increase the amount of the general 8 ~ 10mg / d. ② uracil: uradil (Yupitacin). Non-selective α-blockers are lisdexamfetamine. Prazosin, terazosin, and eupivir are selective blockers, blocking postsynaptic and vascular wall α1 receptors, but not presynaptic and α2 receptors.
(6) Angiotensin II receptor blocker (ARB): Chlorosartan (Kosoya) 50-100mg, 1 time / d, not easy to cause coughing, compliance is good, lowering blood pressure is stable, is conducive to the excretion of uric acid, but is prohibited in pregnant women. This kind of drug in JNC7 has heart failure, diabetes mellitus, chronic kidney disease three strong indications.
(7) Other antihypertensive drugs: such as central sympathetic inhibitors colistin, methyldopa, etc., peripheral sympathetic inhibitors lisdexamfetamine, guanethidine and so on.
(8) Direct vasodilator: hydrazinephenazine, bishydrazinephenazine, 12.5-25mg, 1-3 times / d. Sodium nitroprusside 50-100mg added to 250-500ml of liquid, avoiding the light of the static drip, the number of drops from 5 to 20 drops / min gradually increased, while monitoring blood pressure. Phentolamine 10~20mg added to 250~500mL liquid drip, severe hypertension can be given 10mg static push. In addition, nitroglycerin can also lower blood pressure, 10mg added to 250-500mL of fluid IV.
2. Guidelines for the selection of antihypertensive drugs Antihypertensive drugs should be rationally selected because of their long-term use.
(1) In combination with heart failure, diuretics and ACEI should be used.
(2) For systolic hypertension in the elderly, use diuretics, slow-release or controlled-release agents of calcium antagonists or long-acting agents, such as felodipine and amlodipine.
(3) Diabetes mellitus: mild or moderate impairment of renal function, ACEI, ARB, diuretics are preferred.
(4) Hyperlipidemia: choose α1 receptor blocker, not β2 receptor blocker and diuretics.
(5) Pregnant women should not use ACEI and angiotensin receptor II antagonist, prefer to use methylphenidate.
(6) Bronchial asthma, depression, diabetes mellitus should not use beta-blockers, gout is not suitable for diuretics.
(7) Long-term use of β-blockers should not be stopped suddenly, but gradually, otherwise it may cause sudden death.
(8) Patients with myocardial infarction can use second-generation β-blockers or ACEIs, and calcium antagonists can be used in combination with cardiac angina.
3. Antihypertensive goals
(1) Short-term goal: 140/90 mmHg or less, or 130/85 mmHg or less in young and middle-aged patients (less than 60 years old), as well as those with diabetes or renal changes. For grade 3 hypertension, where the blood pressure is around 220-240/130-150 mmHg or even higher, the first goal of blood pressure reduction is to first reduce the blood pressure by 25% of the original level within 2 hours, maintain it for a certain period of time, and then reduce it to 160/100 mmHg.
(2) Long-term goal: to reduce complications and mortality in target organs such as heart, kidney and brain, and to prolong life.
4.Grade 2 or higher hypertension Most patients need a combination of drugs, as few as two or as many as three to four. Start with a small dose of one drug, gradually increase the dosage if it is not effective, and then add a second drug, also starting with a small dose.
5. Treatment of hypertensive crisis For hypertensive emergencies, treat immediately under.
(1) sodium nitroprusside 50 ~ 100 mg added to 250 ~ 500 ml of liquid in a static drip, avoiding light, 5 ~ 20 drops / min, a few minutes to see the effect, while closely monitoring blood pressure, should not be used for a long time to prevent cyanide poisoning.
(2) Nitroglycerin 10-20mg IV.
(3) Nicardipine 20-40 mg into 500 ml of liquid drip, while observing the blood pressure and adjusting the number of drops.
(4) Urapidil first given 25mg intravenous push, the efficacy is not obvious, repeat injection, and then given 50 ~ 100mg added to 100ml liquid drip.
(5) Phentolamine 10mg IV, then 20-40mg in 250-500ml of fluid IV.
Some patients are particularly sensitive to antihypertensive drugs, and excessive lowering of blood pressure may cause heart, brain, kidney and blood circulation disorders, so it should be moderated.
(6) Complicated with acute left heart failure, at the same time should be given cediran 0.4mg IV or first given 5mg IV, and then given 10mg added to 250ml of liquid IV. If digitalis overdose is suspected, add 20-40mg of dobutamine to the fluid. Tachycardia 20~100mg IV push, oxygen inhalation, can also add aminophylline 0.25~0.5g IV.
(7) Hemodialysis patients often have persistent hypertension, and many of them are volume dependent and should be adequately dehydrated so that medication is effective only when they reach dry weight.
Hypertension refers to the increase of arterial pressure in the body circulation, which can make the systolic blood pressure higher than normal or both high, clinically, hypertension is seen in two types of diseases, the first type is primary hypertension, also known as hypertension, is a kind of blood pressure increase as the main clinical manifestation and the etiology is not yet clear of the independent disease, accounting for the vast majority of all patients with hypertension, the other type is secondary hypertension, also known as symptomatic hypertension, with a clear etiology, it is one of the clinical manifestations of a disease. The other type is secondary hypertension, also called symptomatic hypertension, which has a clear cause and is one of the clinical manifestations of a certain disease, and if the primary disease can be cured, the blood pressure can no longer be elevated.

essential hypertensionIt is caused by a variety of acquired factors on the basis of a certain genetic susceptibility, and there is a clear family aggregation of this disease, which is related to the dysregulation of the balance of the renin-angiotensin-aldosterone system, external mental stimulation, high sodium diet, and insulin resistance.

Pathological features of primary hypertension, small arteriopathy is the most important pathological changes, left ventricular hypertrophy is the most characteristic changes in the heart of hypertension, as well as the central nervous system, renal retina and other small arteries undergo a series of pathological changes.
Primary hypertension can be divided into slowly progressive hypertension and rapidly progressive hypertension according to the course of the disease, and is divided into three stages according to the clinical manifestations. Stage 1: blood pressure reaches the level of diagnosed hypertension, and there is no clinical manifestation of cardiac, cerebral, and renal complications; Stage 2: blood pressure reaches the level of diagnosed hypertension, and there is one of the following: ① Physical examination, X-ray, electrocardiogram, or ultrasound shows left ventricular hypertrophy; ② fundus examination shows general or localized stenosis of fundic artery; ③ proteinuria and/or elevated concentration of creatinine. generalized or localized stenosis; ③ proteinuria and/or elevated plasma creatinine concentration. Stage III: Hypertension reaches the diagnostic level with one of the following: (1) cerebrovascular accident or hypertensive encephalopathy; (2) left ventricular failure; (3) renal failure; (4) fundus hemorrhage or exudation with or without optic nerve papillae edema.
Primary hypertension can reduce cardiovascular and cerebrovascular events (including the occurrence of stroke, myocardial infarction and death) in patients through treatment, and the main purpose of treating this disease is to minimize the risk of damage to target organs such as the heart, brain, and kidneys, as well as the risk of death caused by them, and the treatment methods include non-antihypertensive medication and pharmacological antihypertensive treatment.
secondary hypertensionThe main diseases that cause secondary hypertension are: renal diseases, including glomerulonephritis, pyelonephritis, hypertensive syndrome of pregnancy, renal stones, renal tumors, secondary renal pathology, diabetic nephropathy., etc.; endocrine disorders, such as adrenocortical disorders, hyper- or hypothyroidism, anterior pituitary hyperfunction, etc.; vascular lesions, such as aortic constriction, polyarteritis, etc.; and cranial lesions.
The clinical manifestations of secondary hypertension are mainly the signs and symptoms of the primary systemic disease in question, of which hypertension is only one, and the treatment is mainly directed at the primary disease.
If you find this article helpful, remember to click a like.
To promote medical science, dissect the doctor-patient relationship, and tell doctor-patient stories, please click on the upper right corner and follow my headline number: Anesthesia Superman Man of Steel.
"Happy Little Dawgs" has the answer for you. Joyful Concerns
High blood pressure, I guess we are not strangers to this problem, too unusual, now which people do not have a few people around to get high blood pressure disease? But many people don't know why it is inexplicably targeted. Some people dizziness and other symptoms to come, the first time will also think about this, once diagnosed with high blood pressure, worry about those legendary stroke, heart attack and other "evil" may also not far away from their own.
 Since this thing has been stained, it is natural to want to go to the hospital to figure out why you have this problem, and to get rid of it through some medical means after you understand the cause clearly. However, the reality is that based on the current level of medical development and examination methods, only 5-10% of patients with hypertension can be found out the exact cause of the disease, such as common causes of renal hypertension, endocrine hypertension, renal vascular hypertension and sleep apnea syndrome, in addition to mental and psychological problems can also be seen from time to time caused by high blood pressure. Obviously, there are still almost 90-95% of hypertension whose causes cannot be identified with the current medical conditions, and this part of the population, in which the exact cause of the elevated blood pressure cannot be found, is called primary hypertension.
Since this thing has been stained, it is natural to want to go to the hospital to figure out why you have this problem, and to get rid of it through some medical means after you understand the cause clearly. However, the reality is that based on the current level of medical development and examination methods, only 5-10% of patients with hypertension can be found out the exact cause of the disease, such as common causes of renal hypertension, endocrine hypertension, renal vascular hypertension and sleep apnea syndrome, in addition to mental and psychological problems can also be seen from time to time caused by high blood pressure. Obviously, there are still almost 90-95% of hypertension whose causes cannot be identified with the current medical conditions, and this part of the population, in which the exact cause of the elevated blood pressure cannot be found, is called primary hypertension.
 According to scientific research, it is currently believed that essential hypertension is a multifactorial disease caused by the interaction of certain congenital genes with many pathogenic pressure-boosting and physiological pressure-reducing factors, which mainly include: genetic factors, a high sodium and low potassium diet, overweight and obesity, alcohol consumption, stress, smoking, dyslipidemia, diabetes mellitus, obesity and so on. In layman's terms, that is, if your parents have high blood pressure, then because of genetic inheritance, your chances of getting high blood pressure is much greater than others; if you usually eat habits don't like to mouth fade a bird, such as salted vegetables as the main course to eat, or the main course into a savory like, then your chances of getting high blood pressure is also much greater than the normal dietary habits of the people; of course, if you usually don't Of course, if you usually do not pay attention to exercise, resulting in their own become a big fat, then, high blood pressure is certainly not far from you; in addition, bad habits, such as wine, tobacco, like to eat greasy and sweet, but also a temperament, then congratulations, high blood pressure does not look for you only strange!
According to scientific research, it is currently believed that essential hypertension is a multifactorial disease caused by the interaction of certain congenital genes with many pathogenic pressure-boosting and physiological pressure-reducing factors, which mainly include: genetic factors, a high sodium and low potassium diet, overweight and obesity, alcohol consumption, stress, smoking, dyslipidemia, diabetes mellitus, obesity and so on. In layman's terms, that is, if your parents have high blood pressure, then because of genetic inheritance, your chances of getting high blood pressure is much greater than others; if you usually eat habits don't like to mouth fade a bird, such as salted vegetables as the main course to eat, or the main course into a savory like, then your chances of getting high blood pressure is also much greater than the normal dietary habits of the people; of course, if you usually don't Of course, if you usually do not pay attention to exercise, resulting in their own become a big fat, then, high blood pressure is certainly not far from you; in addition, bad habits, such as wine, tobacco, like to eat greasy and sweet, but also a temperament, then congratulations, high blood pressure does not look for you only strange!
 Some people may not care about this problem, especially in the 30s and 40s of young and middle-aged (yes, this is the age group, younger patients with high blood pressure is also very common), that not much, not to mention let them take antihypertensive medication, even changes in lifestyle are unlikely to be, so ah, this part of the people, basically in the chronic suicide, I work in hospitals, thirty-four years old to get a cerebral infarction, cerebral hemorrhage, I work in a hospital, thirty-four-year-old cerebral infarction, cerebral hemorrhage, heart attack is really not rare, some unlucky children, sent to the intensive care unit may not be able to save, leaving orphans, widows and mothers, as well as the old man sad.
Some people may not care about this problem, especially in the 30s and 40s of young and middle-aged (yes, this is the age group, younger patients with high blood pressure is also very common), that not much, not to mention let them take antihypertensive medication, even changes in lifestyle are unlikely to be, so ah, this part of the people, basically in the chronic suicide, I work in hospitals, thirty-four years old to get a cerebral infarction, cerebral hemorrhage, I work in a hospital, thirty-four-year-old cerebral infarction, cerebral hemorrhage, heart attack is really not rare, some unlucky children, sent to the intensive care unit may not be able to save, leaving orphans, widows and mothers, as well as the old man sad.
Of course, don't panic when you see this, although for the time being you can't figure out what the hell is going on when you get high blood pressure, it's not like there's no way to deal with it. A healthy lifestyle, at all times, is an effective treatment for any person with high blood pressure (including normal high-value blood pressure) to lower blood pressure and control other risk factors and clinical conditions. How to do this, as mentioned above, is to reduce sodium intake and increase potassium intake; control body weight; do not smoke; do not drink alcohol in excess; exercise; reduce mental stress and maintain psychological balance. In addition, some hypertensive patients take medication is difficult to avoid, some people are afraid that once you start taking medication, you can't stop for life, but there is no way, if the blood pressure is not well controlled, resulting in more troublesome problems, then you may have to take more medication to solve these troubles, and even the opportunity to take medication is gone, how would you choose.
When to start taking the medication, what to take and how to take it, I won't tell you all about it here, my advice is to go to the hospital and see your doctor, they will tell you all about it.
In short, mind your own business and listen to your doctor, then you don't need to panic and I hope everyone is always healthy!
"Happy little doctor" every day for you to push the health of medical knowledge, sharing cases, do not forget to click on the upper right corner of the attention yo!
Primary hypertension, which is simply understood to be what we usually refer to as high blood pressure, accounts for almost 95% of hypertension.
In other words these high blood pressures don't really have a direct cause found, they are just high blood pressures without a cause.
So some of you have asked, isn't it true that high blood pressure is related to many factors?
Yes, high blood pressure is related to many factors, but to just these factors can lead to high blood pressure, but are not the direct cause of high blood pressure.
Let's start with secondary hypertension, so-called secondary hypertension is all about clear causes, such as renal artery stenosis, pheochromocytoma, renal failure, primary aldosteronism, and so on.
As long as we remove these causes, then these high blood pressures can be cured, for example, pheochromocytoma is operated on and the blood pressure is normalized, for example, renal artery stenosis is operated on and the blood pressure is normalized.
But when we say primary hypertension, most of them need to be controlled by antihypertensive drugs, but we also said above that although there is no direct cause of primary hypertension, there are many indirect causes, such as: smoking and drinking, obesity, high salt diet, no exercise, staying up all night, high stress, genetic reasons and so on.
Therefore, we face primary hypertension has always emphasized: quit smoking and drinking, adhere to aerobic exercise, low-salt diet, avoid staying up late, reduce stress and other healthy lifestyle. The control of these indirect causes is the foundation of controlling primary hypertension!
(Dr. Cardiovascular Wang officially authorized original protection, such as theft must be held legally responsible.)
Hypertension is a very common disease in modern times. Adults (≥18 years of age) are defined as hypertensive if their arterial systolic blood pressure is ≥140 mmHg (18.7 kPa) and/or diastolic blood pressure is ≥90 mmHg (12.0 kPa) when measured by a sphygmomanometer according to the regulations in a quiet state.
We generally categorize hypertension into primary hypertension and secondary hypertension, of which secondary hypertension refers to hypertension caused by certain reasons or diseases, commonly renal artery stenosis, adrenal tumors, hyperthyroidism, etc., which generally accounts for about 5% of hypertension.
The remaining 95% of high blood pressure whose cause is not fully understood is called primary hypertension. Its occurrence is related to a number of factors, such as heredity or eating more salt, adrenaline secretion, abnormalities in the XX system, and so on. Regardless of whether it is primary or secondary hypertension, blood pressure should be controlled at a normal level so as to minimize target organ damage and reduce the risk of hypertension.
This question and answer are from the site users, does not represent the position of the site, such as infringement, please contact the administrator to delete.